Since the introduction of duplex ultrasound, there has been an explosion of research articles studying many different parameters of the reflux phenomenon. These include reflux duration, peak reflux velocity, and volume displacements, which are ways of quantifying the severity or intensity of reflux.
Superficial venous reflux can be explained as retrograde flow of a column of blood in continuity with a normal competent venous system. It is considered pathologic if it lasts > 1 second. For reflux to occur, a conduit is required together with a provocation maneuver.
The conduit consists of one or more upper feeding points, a refluxive pathway, and lower drainage points. Studies on the mechanism of refluxive filling and cessation are fundamental in the understanding of venous insufficiency because reflux cessation is the primary aim of all the treatment strategies.
The majority of clinically relevant venous refluxes of the superficial veins requiring invasive treatment occur in the great saphenous vein (GSV) territory.
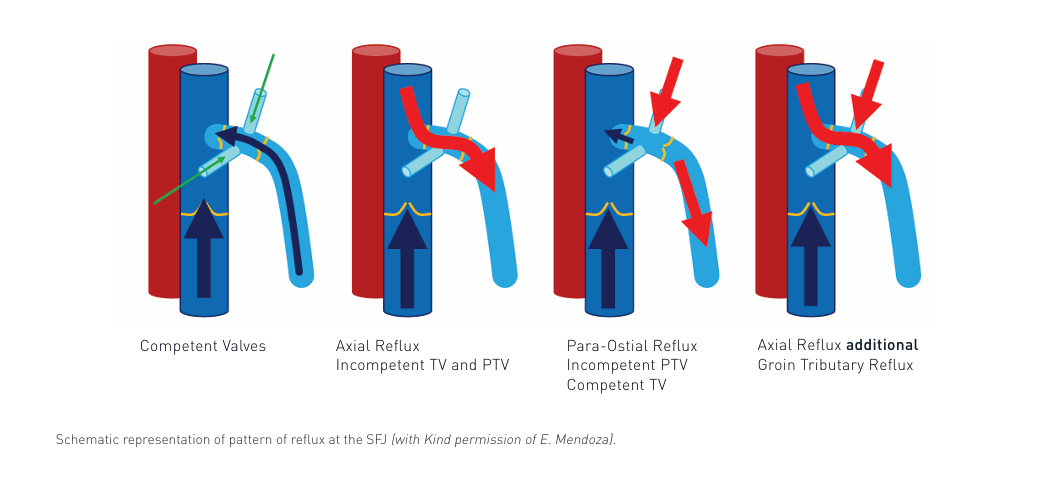
The GSV, similarly to other veins, is equipped with valves that preclude venous reflux, i.e. a backward flow. In the area of the SFJ two valves are especially important: the terminal valve, which is located next to the junction with the femoral vein, at a mean distance of 0.4 cm from the junction, and the preterminal valve, which is located more distally from the SFJ, usually at
a distance of sev- eral centimetres from the femoral vein and distally from the above-mentioned tributaries.
Venous anatomy of the region should be evaluated and several questions should be answered:
• Are all veins visible?
• Are the valves of the GSV visible, and are their leaflets capable of moving during the blood flow
• Are the valves of the SFJ competent?
• Which tributaries are visible?
• Is the GSV dilated?
Assessment of venous flow in the area of the SFJ should preferentially be performed in the standing position.
The provocation maneuver can be pressure from above, like the Valsalva maneuver, or a calf release or toe elevation maneuver from below.
In a case of incompetent valves of the SFJ an upward flow during muscular systole and backward flow during diastole will be found, with duration of such a backward flow longer than one second. Flow characteristics in the area of SFJ: in the CFV, and the GSV and its tributaries can be assessed using colour Doppler mode. Flow characteristics should be documented in the
CFV, and the SFJ and tributaries using PW-Doppler mode.
DUS examination should be performed:
• Standing
• Morphology Longitudinally and Cross Section
• Colour Duplex Exploration: Reflux source, reflux path, PW to document the findings
• Manoeuvres: At least two out of Valsalva, Toe elevation and Calf compression


